
Bedsharing and sudden infant death (SIDS) risk
Sarah Ockwell-Smith, Professor Wendy Middlemiss, University of North Texas, Tracy Cassels, University of British Columbia, Helen Stevens, and Professor Darcia Narvaez, University of Notre Dame. Adapted from an essay in The Science of Mother Infant Sleep.
In 2013, a meta-analysis by Carpenter et al. examined the risk factors for sudden infant death syndrome (SIDS). The objective was to resolve uncertainty as to the risk of SIDS associated with sleeping in bed with your baby if neither parent smokes and the baby is breastfed. While we commend the authors for examining those risks associated with incidence of SIDS, we question their conclusion that a substantial reduction in SIDS rates could be achieved if parents avoided bedsharing and consider that conclusion unsubstantiated. Their analysis used faulty and missing data, and they did not account for confounding criteria (used to define bedsharing and risks)—an important challenge in any meta-analysis.
Carpenter et al. examined some of the most salient risk factors for SIDS events:
- infant sleep position
- parental cigarette smoking
- infant birthweight
- age
These risks have previously been well documented as contributing significantly to an increase in risk of SIDS events. It is not surprising to note that these factors remain risks in a re-evaluation of the findings.
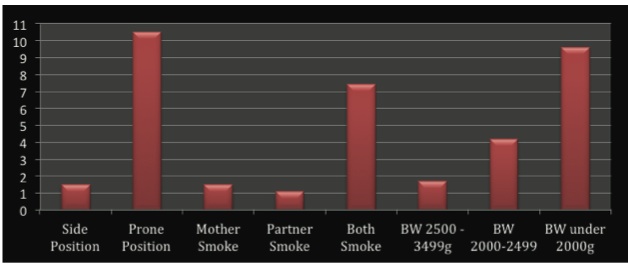
While those risks examined contribute to the possibility (see Chart 1 below), so too do other factors (see below for a list of risks not considered). Without consideration of additional risks, it is not possible to determine that one variable, bedsharing in itself, is inherently responsible for risk remaining in this meta-analysis. Nor is it possible to say that one of the variables within the nighttime care routine, such as breastfeeding, is not protective.
Chart 1. Adjusted Odds Ratios from Carpenter et al. (2013)
Major limitations
Treatment of breastfeeding
Buried deep in the last section of the paper is the recommendation that breastfeeding be supported as a mechanism for protecting infant health.
Chart 2. Adjusted Odds Ratios including bottle-feeding from Carpenter et al. (2013)
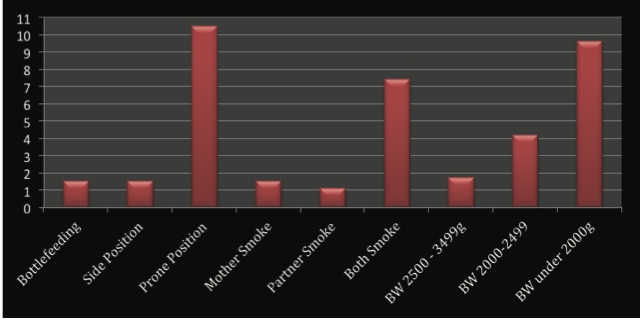
Note: BW = birthweight
In examining the role of breastfeeding, the authors overlook an essential aspect of infant development: breastfeeding contributes positively to both immediate and later infant health outcomes, not just a reduction in SIDS, though it serves as a protective factor there as well (Alm et al., 2002; Ford et al., 1993; Horne et al., 2004; McVea et al., 2000; Mitchell et al., 1992; Mosko et al., 1997; Scragg et al., 1993). It is important from any perspective to encourage breastfeeding through the infant’s first year of life (UNICEF, Victoria, C. et al., 2016). Carpenter et al. couch the protective factor of breastfeeding in the arena of risk, thus confusing the message for practitioners and parents.
Instead of looking at how each of the variables in the dataset may contribute to risks with infants’ breathing or how they may compromise arousal, the authors focus on whether the act of breastfeeding protects against all risk of SIDS. Clearly, that is a standard that cannot be reached. Regardless of parental behavior, without the necessity of meta-analyses, the imputing of data from 5 of 12 variables, the compromising operational definitions of nighttime care contexts, we can say breastfeeding is protective. There is still a risk because there are multiple risk factors that compromise infants’ capacity to breathe and infants’ ability to arouse. Breastfeeding does not vaccinate against all risks (e.g., a pillow in the face).
The authors overlook the Adjusted Odds Ratios (AOR) for bottle-feeding and SIDS risk. The authors pay lip service to breastfeeding, but suggest that bedsharing to encourage breastfeeding is ill advised. They cite the Netherlands as a key example of how an active campaign to discourage bedsharing has lowered the rates of SIDS and confirm that promotion of bedsharing is not necessary to achieve high rates of prolonged breastfeeding. They fail to establish their point here, given the relatively low rates and increases over the 10-year period discussed (a rise of 7% and 8% of any breastfeeding at 3 and 6 months, respectively). Perhaps the anti-bedsharing campaign inhibited greater growth in breastfeeding, something that should be of concern when examining the costs associated with infant health. In the U.S. alone, a cost-analysis found that if we could get 80% mothers to breastfeed exclusively for six months (the WHO recommendations), the U.S. would save $10.5 billion a year in health-related costs (Bartick & Reinhold, 2010). In 2016 Victoria et al. reported on the most extensive piece of research into the effects of breastfeeding ever undertaken. Increasing breastfeeding worldwide could prevent 800000 child deaths. Failing to breastfeed costs the global economy around US$ 302 billion every year.
Furthermore, it is misguided to argue that if bedsharing were recognized as a means of supporting breastfeeding that we would see more SIDS events. Even more dangerous is to abandon support of breastfeeding in favor of supporting breastfeeding only if it detours bedsharing. Although the AOR in the current meta-analysis suggests that bottle-feeding is a lower risk factor than bedsharing (the validity of which will be discussed below), it only concerns itself with SIDS events, not the protective benefits of breastfeeding on infant health, of which there are many, both immediate and long term (Horta et al., 2007; Ip et al., 2007; Martin et al., 2005; Owen et al., 2002). To only consider SIDS events ignores the effects of lower breastfeeding rates on myriad other diseases.
Risk factors not included in the analysis
The authors have confirmed some of the major risk factors associated with SIDS, both independently and when interacting with sleep location: sleep position, parental smoking, alcohol use, drug use, birthweight, and infant age. The authors solidified many risks, as they were stated individually in the reports associated with each large data set. With this, researchers, practitioners, and parents now have a clear documentation of these specific risks. They clearly confirmed the known risks and quantification of those risks. For example, maternal smoking remains to be one of the most salient risks associated with SIDS—with paternal smoking contributing to risk as well. Similarly, infant sleep position (i.e., prone and side sleep), contribute significant risk for SIDS events.
Missing from the analysis however are other known risk factors that are recognized as part of the triple-risk model:
- critical developmental period (infant age)
- environmental context (bedding)
- infant vulnerability (prematurity).
Additionally, the authors fail to include data sets that do examine these risk factors and that come to very different conclusions about the inherent risk of bedsharing on SIDS events (e.g., Blabey & Gessner, 2009). The authors argue that bedsharing is causally related to SIDS events via theories about infant breathing and arousability. Specifically, the authors state that , “[t]he proposition that bedsharing is causally related to SIDS is coherent with theories that respiratory obstruction, re-breathing expired gases, and thermal stress (or overheating), which may also give rise to the release of lethal toxins, are all mechanisms leading to SIDS, in the absence of smoking, alcohol or drugs. Infants placed prone are exposed to similar hazards.” Is the implication that breastfed, bedsharing babies are at inherent risk of SIDS events verifiable? The answer is equally as simple, but much more informative: No.
Again, factors that put infants’ breathing and arousability at risk also increase the risk of SIDS events. The elements of the sleep context that place infants’ breathing and arousability at risk are well defined:
- respiratory obstruction (e.g., bedding)
- rebreathing expired gases (i.e., from cover on face)
- thermal stress through overheating (e.g., too many covers)
- physiological vulnerability of arousal (e.g., deep sleep from formula usage)
The authors seem to be arguing that parenting behavior which can be associated with risk, even if the source of risk is not the behavior, should be stopped (i.e., bedsharing). This is problematic, given that bedsharing is a universal, evolved practice, and is often preferred by parents. The absence of bedsharing does not eliminate risk of SIDS events. The diminishing of bedsharing is certainly associated with decreases in the protective behavior of breastfeeding.
A nighttime care context that includes bedsharing and breastfeeding can include elements that compromise infants’ breathing and ability to arouse. Importantly, we know that breastfeeding not only does not contribute to the risk, but serves to help reduce these risks. See Table 1: bottle-fed infants are at a greater risk of a SIDS, regardless of sleep location.
What about bedsharing?
The authors would have us believe bedsharing per se increases the risk of compromising infant breathing and arousability. However, they fail to acknowledge that there are other factors that influence breathing and arousability such as:
- bedding
- temperature
- premature status (which is correlated with birthweight, but carries with it unique risk factors that must be considered).
Data from Alaska between 1993 and 2004 examined the same question of bedsharing risk, only they also included other known risk factors, such as sleep surface (not just sofas, but the type of bed) and sleeping with a non-caregiver, and compared the data not just to controls (Blabey & Gessner, 2009). Additionally, the comparison group was taken from a state-wide monitoring system that does not focus on answering one day of bedsharing habits, but rather, asks parents about usual bedsharing habits. As such, they most likely had more accurate information on bedsharing than the studies included in the current review. What was found in Alaska? Of the SIDS events that took place while bedsharing, 99% included at least one risk factor, and thus, the authors concluded that “infant bedsharing in the absence of other risk factors is not inherently dangerous.”
So, instead of looking at secondary issues, let’s focus on discussion of the primary issue: decreasing the risk of SIDS events. If we want to decrease risk of SIDS events, then we must ensure infants are in the best possible situation to support breathing and arousability.
How to do that?
Address maternal and infant health that reduces risk
- Reduce elements that contribute to vulnerability prenatally:
- intrauterine exposure to cigarette smoke
- premature birth
- low birthweight
- stressful pregnancy with increased cortisol in blood stream
- Reduce vulnerability postnatally by increasing health:
- through breastfeeding
- increasing proximity to parent during sleep to protect arousability
- increase supportive contexts within which to support new parents with breastfeeding, infant and maternal health. (This support will decrease infant vulnerability, increase infant health and the capacity to arouse.)
- Increase maternal nutrition during pregnancy
- Address nighttime care practices to help ensure breathing and arousability:
- Place infants on their back to protect breathing
- Protect infants’ breathing and arousal by having infants sleep on a firm, flat surface without pillows, toys, or blankets
- Protect infants’ arousal response by having a cool sleep environment, absent of blankets
- Continue to monitor sleep space:
- Keep infants in close proximity to parents to ensure awareness of compromised breathing or arousal response that may be associated with unobservable variables, such as immature physiological responses
Despite a long history of efforts to reduce bedsharing, this nighttime-care practice remains the preferred practice of many, is increasing in some areas, and provides many protective or health-benefiting outcomes for mothers and infants. The close interaction between breastfeeding and bedsharing is well documented as is the association between bedsharing and greater duration of breastfeeding. Infants’ safety at night is compromised when discussions shift from the criteria above to admonitions to sleep separately. A focus on protection and a discussion of what underlies risk will be much more successful in reducing risk of SIDS, as well as improving the health context postnatally.
Ten important risk factors that are missing from Carpenter et al. (2013) |
|
| 1 | The researchers importantly did not consider whether the bedsharing was planned. Previous research from Venneman (2009) showed no increased risk in planned bedsharing (versus unplanned). This is an incredibly important omission. |
| 2 | The paper did not consider the effects of the mother smoking during pregnancy, only smoking post birth. |
| 3 | Breastfeeding information is too limited to draw conclusions. No difference has been drawn between frequency and percentage of breastfeeds versus formula feeds for those “partially feeding.” |
| 4 | The paper only considered illegal drug use. Many postnatal mothers (0-12weeks after the birth) are prescribed analgesic medication for related birth-induced injuries, including, but not limited to, Caesarean healing, known to have a sedative effect. This was not considered at all. |
| 5 | Prematurity was not considered at all. |
| 6 | Parental exhaustion was not considered at all. Some experts suggest this is considered to be less than 4-5 hours of sleep in the past 24-hour period, other experts advise parents to use their instincts. Parental exhaustion naturally impacts on responsivity to infant cues. |
| 7 | The researchers did not examine the effect of maternal (and paternal) obesity. |
| 8 | No differentiation was made between having one or both parents in the bed and more importantly, the location of the baby. It is advisable that the mother sleeps in between the father and infant. Equally, it was not noted if older siblings were also present in the bed. |
| 9 | The researchers did not fully consider the impact of alcohol consumption by the father when bedsharing. |
| 10 | No mention was made of whether parents were aware of the risks of bedsharing and how to minimize these before sharing a bed with their infant. |
Resources
ISIS: Infant Sleep Information Source: Bed-Sharing and Safety
ISIS: Infant Sleep Information Source: Key Research 2014 to 2016
ISIS: Infant Sleep Information Source: Normal Infant Sleep
UNICEF: The Breastfeeding Friendly Initiative: Caring for Your Baby at Night
UNICEF (2016): Bed Sharing, Infant Sleep and SIDS
References
, et al. (2002). Breast feeding and the sudden infant death syndrome in Scandinavia 1992–95.
Blabey, M.H., & Gessner, B.D. (2009). Infant bed-sharing practices and associated risk factors among births and infant deaths in Alaska. Public Health Reports, 124, 527 -534.
Carpenter, R., McGarvey, C., Mitchell, E.A., Tappin, D.M., Vennemann, M.M., Smuk, M., & Carpenter, J.R. (2013). Bedsharing when parents do not smoke: Is there a risk of SIDS? An individual level analysis of five major case-control studies. British Medical Journal Open, BMJ Open 2013;3:e002299. doi:10.1136/bmjopen-2012-002299
Ford, R.P.K., Taylor. B.J., Mitchell, E.A., et al. (1993). Breastfeeding and the risk of sudden infant death syndrome. International Journal of Epidemiology, 22, 885- 890.
Horne, R.S., Parslow, P.M., Ferens, D., Watts, A.M., & Adamson, T.M. (2004). Comparison of evoked arousability in breast and formula-fed infants. Archives of Diseases of Childhood, 89(1), 22-25.
Horta, B.L., Bahl, R., Martinés, J.C., et al. (2007). Evidence on the long-term effects of breastfeeding: Systematic review and meta-analyses (pp. 1-57). Geneva: World Health Organization.
Ip, S., Chung, M., Raman, G., et al. (2007). Breastfeeding and maternal and infant health outcomes in developed countries. Evid Rep Technol Assess (FullRep), 153, 1-186.
Martin, R.M., Gunnell, D., & Smith, G.D. (2005). Breastfeeding in infancy and blood pressure in later life: Systematic review and meta-analysis. American Journal of Epidemiology, 161, 15-26.
McVea, K.L., Turner, P.D., & Peppler, D.K. (2000). The role of breastfeeding in sudden infant death syndrome. Journal of Human Lactation, 16, 13-20.
Mitchell, E.A., Taylor, B.J., Ford, R.P.K., et al. (1992). Four modifiable and other major risk factors for cot death: the New Zealand study. Journal of Paediatric of Child Health, 28(suppl 1), S3-S8.
Mosko, S., Richard, C., & McKenna, J. (1997). Infant arousals during mother-infant bed sharing: implications for infant sleep and sudden infant death syndrome research. Pediatrics, 100, 841- 849.
Owen, C.G., Whincup, P.H., Gilg, J.A., et al. (2003). Effect of breast feeding in infancy on blood pressure in later life: systematic review and meta-analysis. BMJ, 327, 1189-1195.
Owen, C.G., Whincup, P.H., Odoki, K., Gilg JA, Cook DG. (2002). Infant feeding and blood cholesterol: a study in adolescents and a systematic review. Pediatrics, 110, 597- 608.
Scragg, L.K., Mitchell, E.A., Tonkin, S.L., & Hassall, I.B. (1993). Evaluation of the cot death prevention programme in South Auckland. New Zealand Medical Journal, 106, 8-10.
Victora, C. et al. (2016) Breastfeeding in the 21st century: epidemiology, mechanisms, and lifelong effect The Lancet, 387(10017), 475-490.



















5 Pingback