
Teresa Pitman explains what’s behind a baby’s instinctive knowledge.
Adapted from Preparing to breastfeed: A pregnant woman’s guide
Most mothers imagine breastfeeding is something they do. Moms figure out when it’s time to feed again, they bring the baby to the breast, they put the nipple in the baby’s mouth, they make sure the latch is good, and unlatch the baby when the feeding is done.
The truth is, your baby knows a lot more than most people imagine about breastfeeding. He’s born with the instincts and skills to make breastfeeding work, just like other baby mammals are. (If you’ve ever seen a cat with newborn kittens or a baby calf with its mother, you’ll know that they are clearly hardwired to find food. Our babies are too.) Of course, mothers also have built-in skills for breastfeeding, and those mesh nicely with the baby’s.
Human babies aren’t as physically strong and capable as some others. That baby calf can walk and run within hours of birth—your baby won’t be walking for year or so. That’s a big difference! Our babies need more help from their mothers. Mama cow just has to stand still while her baby latches on; you may need to do a bit more than that. But maybe not as much as you think.
Where a baby wants to be
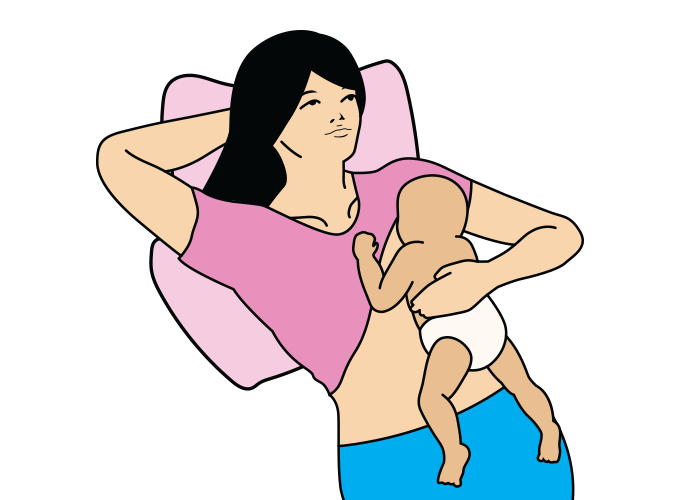
If someone hands you a fussy baby, what do you do? Most women, without even thinking about it, will hold the baby vertically against their chest or shoulder, with baby’s tummy against their chest, one hand behind baby’s shoulders and the other behind his bottom. This natural position for soothing is also the perfect spot for the baby to begin feeding.
What typically happens is that the baby will first snuggle into your chest a little, and then will lift up his head, or even throw his head back. Sometimes parents think this is because the baby’s neck muscles aren’t very strong, or imagine it’s just a random movement, but researchers who have observed many babies tell us that it’s deliberate. It seems to be part of the way the baby orients himself when in contact with his mother’s body: “Hmm, let’s look around and see where I am—yup, there is her head, so those nice things with the milk in them should be a little lower, one on either side.” And, in fact, if your baby is hungry, what he’ll do next is move to one side or the other, heading towards the breast. Some babies do this very vigorously—they practically throw themselves sideways. Others squirm or wiggle to one side.
Watch this video to see how much a newborn knows!
Some experts feel that when we pick up a crying newborn and hold him in what we think of as a breastfeeding position (horizontally across our tummies, head toward the breast) that we are actually confusing the baby. His instinctive expectation is to be held vertically, in that soothing position, so that he can find his own way to the breast. (Of course, older, more experienced babies are less concerned—once they’ve mastered breastfeeding, they don’t mind at all being moved into position.)
Nurses, lactation consultants, and others have used a variety of techniques to help mothers get their babies properly positioned and attached to the breast. There’s more detailed information on different approaches in my book. Many breastfeeding experts encourage mothers to start with “laid-back breastfeeding,” which just means getting into a comfortable, semi-reclining position, baby tummy-down on your chest, and letting the baby find the breast to latch himself on, helping as required. He can get a good, deep latch, with the nipple well back in his mouth. (In more upright positions, the baby is reaching up to the nipple, and it’s easier to just latch on to the nipple, not the breast.) Some find this ideal to start, comfortable and restful, while you are working together to get breastfeeding going.
Making milk and varying feeding patterns
Your baby doesn’t know the mechanics of milk production and how the breast functions, but he knows exactly how to establish a good milk supply, how to adjust the milk supply to meet his needs, and how to change the fat content and other components of the milk as his needs change over time. All you have to do is follow his lead.
One of the significant differences between formula and human milk is that formula is always the same (unless, of course, the manufacturer finds a cheaper type of oil to add to it, for example), while human milk changes at every feeding:
- Sometimes it has more of a certain type of antibody, for example, or more fat.
- Milk produced in the evening or night has components that help to relax the baby and encourage sleep.
- If the mother has eaten something highly flavored, garlic for instance, the flavor comes through in the milk.
We don’t always understand the purpose of all these changes, but many of them are clearly important for the baby. The baby varies his feeding patterns to make sure the milk he gets is meeting his needs. Let’s say he’s going through a period of rapid brain growth, then he needs more of the fats in the milk that build brain cells. Frequent, short feedings will bring him more of that high-fat milk.
Or let’s say it’s a hot day and your baby needs more liquids. He may go a bit longer between feedings, and then want to switch quickly from one breast to the other, so he gets more of the lower-fat milk to quench his thirst.
Maybe there is a virus going around. You and your baby have both been exposed to it. As your baby starts to feel a bit ill, he nurses more often to maximize the antibodies and immune factors he will get from your milk to reduce the impact of the illness.
As a new breastfeeding mother, there may be many times that you wonder, “Why is my baby feeding so often today?” or “Hmm, what’s causing him to nurse less often this afternoon than usual?” Often there is no obvious answer. Trust that your baby knows what he’s doing. He’s adjusting the components of your milk and your milk production to meet his ever-changing needs. All you have to do is recognize his cues and feed him when he asks.
You can see why it’s a problem when mothers react to these high frequency days—as sometimes happens—by assuming they are no longer making enough milk for their baby and giving him a supplement instead. Now he’ll be full, true, but instead of getting signals to make MORE milk, the breasts will fill up more slowly and respond by making LESS milk.
The baby gets more frustrated when he goes back to the breast because he was trying to increase his milk supply, not decrease it. He tries to nurse even more often. The mother is more convinced than ever that something is wrong with her milk supply (why else would her baby be nursing all the time?), and increases the supplement. Her milk production drops even more. Soon her concern becomes reality, and she doesn’t have enough milk to satisfy her baby. She would have had, though, if she’d let her baby demonstrate his skill at increasing milk production.
Sometimes mothers who are having difficulties breastfeeding are told—by nurses, midwives, friends, family, and others who are helping or supporting them—that their babies are lazy, stubborn, or not trying. Sometimes mothers feel that their babies are rejecting them, that they refuse to take the breast because they don’t like it, or don’t want to breastfeed, or, worst of all, that they don’t like their mothers. NONE OF THESE THINGS IS TRUE!
If you offer your baby the breast and he doesn’t latch on, it’s not because he’s stubborn or lazy or mad at you. And it’s most likely not because there’s something wrong with him. He’s a baby. He is hardwired to breastfeed; breastfeeding is so important to the survival of the human species that it couldn’t possibly be relegated to something only “compliant and hard-working” babies do.
The baby who “won’t” breastfeed. It’s not that he doesn’t want to, he does. (Or he would if he was able to think that way. He’d want all the good things that breastfeeding offers—the closeness and comfort, the optimal development, the antibodies and immune support. But he doesn’t know about those things. All he knows is that every cell in his body tells him to find the breast and get milk.)
So why can’t he breastfeed? Well, there are many possible reasons, including the following.
- Your breast may be engorged because of intravenous fluids given during labor, or you may have very large breasts or flat nipples and need more ideas for positioning your baby comfortably because he still has a tiny mouth.
- Medications given in labor may be affecting his ability to find the breast, latch on, and coordinate sucking and swallowing. Breastfeeding, while simple in some ways, requires some complex abilities on the baby’s part.
- He’s had some negative experiences and is trying to protect himself. Perhaps he had deep suctioning of his mouth and airways at birth and found that traumatizing—so he’s avoiding opening his mouth at all. Or perhaps the first few times he was held in a breastfeeding position, someone pushed his (possibly sore from the birth) head into the breast, and he’s afraid that will happen again. (Your own negative experiences play a big part too. It’s easy for a vulnerable new mother to lose all confidence.)
- He’s learned something different. Maybe his first feeding or two was given via bottle. He’s a smart kid: he quickly figured out that food comes from those firm plastic things, and that’s what he’s looking for when he’s hungry. Now you offer him a soft, warm breast with a smaller, softer nipple. He thinks it’s nice, but has no idea that this could also be a food source.
- In a small number of cases, there are physical issues making breastfeeding hard for him and your physician may need to examine either or both of you.
Yes, he does want to breastfeed
Babies need help and patience to resolve problems, so they can breastfeed successfully. Right from the start, your baby knows and loves you. Talk to him, even in a room with a dozen other voices, and he’ll turn toward the sound of your voice. Express a little of your milk onto a breast pad, and he’ll turn his head towards it rather than a breast pad with some other woman’s milk on it.
The job of people who are helping you with breastfeeding is to make it possible—not to criticize him or label him. He really is doing the best he can, and so are you.
One of the phrases I heard that made a difference for me was “trust your baby, trust yourself.” It helped me a lot then, and it is still a good piece of advice today. Yes, there may be times when you need extra help and support, but you and your baby already both know a lot about making breastfeeding work.
Teresa Pitman mother of four and grandmother of ten lives in Canada and has been supporting mothers for more than 35 years with birth and breastfeeding. She is a prolific writer and popular speaker, much loved by all whose lives she touches.
 More posts by Teresa on Women’s Health Today:
More posts by Teresa on Women’s Health Today:
3 Ways for a New Mother to Mother Herself
Birth Interventions and the Impact on Breastfeeding
Helping Premature Babies to Breastfeed



















Leave a comment